Most disc pain is not surgery pain
Many MRI disc bulges are old or incidental. Surgery usually targets nerve compression, instability, or a structural pain generator that matches the symptoms and exam.
Lumbar L5/S1 and L4/5. Cervical C5/6 and C6/7. Plain English first.
A practical guide to back and neck pain when a disc might be involved: symptoms, MRI diagnosis, emergency warning signs, non-surgical care, microdiscectomy, artificial discs, spinal fusion, recovery, risks, costs, and how to find the right specialist near you.
Many MRI disc bulges are old or incidental. Surgery usually targets nerve compression, instability, or a structural pain generator that matches the symptoms and exam.
Leg pain below the knee, numbness, tingling, weakness, and a positive straight-leg raise can point toward lumbar radiculopathy.
Most lumbar disc herniations occur at L4/5 or L5/S1. Cervical radiculopathy commonly involves C6 and C7 roots from C5/6 or C6/7 disease.
Fusion may help instability or severe degenerative collapse, but it is not a simple upgrade from discectomy. It changes motion and carries implant and adjacent-level risks.
Demographics and burden
The difficult part is separating the huge number of people with back pain from the smaller group with a surgically meaningful disc, nerve, stenosis or instability problem.
WHO estimates cases may rise to 843 million by 2050. Low back pain is the leading cause of disability worldwide, but about 90% is non-specific rather than a clear surgical disease.
CDC/NCHS 2019 data found back pain was the most common pain site. It rose from 28.4% at ages 18-29 to about 44-46% after age 45, and was slightly more common in women.
Herniated nucleus pulposus is often cited at 5-20 cases per 1,000 adults annually, with men affected more often. Symptomatic lumbar disc herniation is commonly estimated around 1-3% of people.
In this age range, most lumbar herniations are at L4/5 or L5/S1. Above those levels becomes relatively more common later in life as degeneration, stenosis and deformity enter the picture.
Registry studies show large variation: 29 per 100,000 in Sweden, 46 in Denmark and 58 in Norway during 2011-2013, with older international estimates from 14 in Great Britain to 70 in the US.
JAMA analyses placed low back and neck pain among the costliest US health conditions. UK analyses estimate about GBP 12B when health-care costs and lost productivity are combined.
Back pain overview
The spine is a stack of discs, bones, joints, ligaments, muscles, nerves and tissues that can become inflamed. Several problems can look similar on day one, and several can coexist on the same MRI.
A disc is more likely to be clinically important when pain travels in a nerve pattern, there is numbness, reflex change, weakness, a matching MRI finding, and symptoms fail to settle with time, physiotherapy, medication, or injections.
Emergency red flags
New urinary retention or incontinence, loss of bowel control, saddle numbness around the genitals or anus, or bilateral sciatica can signal nerve compression needing emergency MRI and surgical review.
Rapidly worsening leg or arm weakness, clumsy hands, new gait imbalance, falls, or a central cervical or thoracic disc protrusion pressing on the spinal cord is urgent.
Fever, recent infection, immune suppression, IV drug use, known cancer, unexplained weight loss, severe night pain, osteoporosis, steroid use, or major trauma changes the workup.
Diagnosis and imaging
Best routine test for discs, nerve roots, stenosis, cord compression, infection, tumor and postoperative scarring. The key is matching the image to the story and neurological exam.
Useful for bone detail, calcified disc, fracture, surgical planning, and when MRI is not possible. CT myelography is sometimes used when metalwork or MRI limits clarity.
Plain films show alignment, scoliosis, spondylolisthesis, instability and hardware. Flexion-extension views may matter when fusion is being considered or after surgery.
Not routine for ordinary herniated discs. They may help when clinicians suspect infection, malignancy, inflammatory disease, occult fracture, active facet pain, painful hardware, or another inflammatory pain generator.
A straightforward herniation in an otherwise less chaotic-looking spine is easier to teach from. Real patients, however, often bring older injuries, degeneration, previous surgery, slippage, inflammatory pain generators and incidental findings into the same appointment.


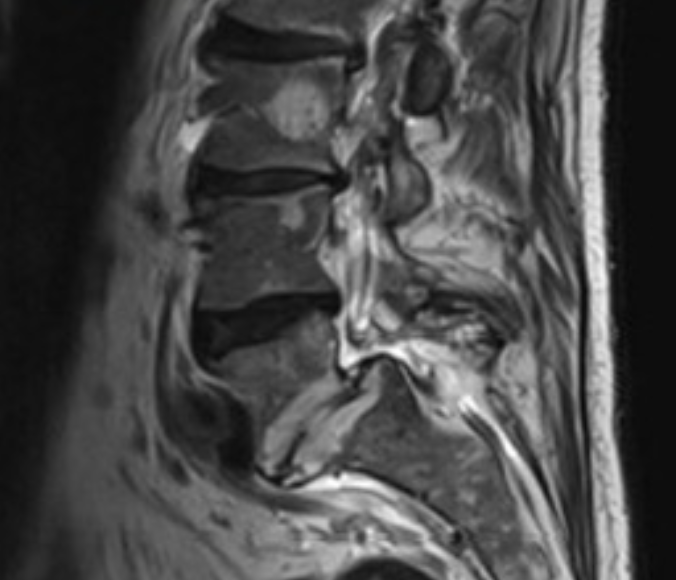
A sagittal image looks from the side and helps clinicians count levels, compare disc height, see the canal and look for slippage, collapse or central compression. An axial image cuts across one level and shows the canal, lateral recesses and foraminal routes where nerve roots can be crowded.
This example is the author's spine, roughly 28 years after L5/S1 disc surgery, and is more complicated than a simple one-level herniation: the L5/S1 disc space has effectively been lost or removed, with spondylolisthesis and a pars defect also in the story. A higher vertebral hemangioma can also be seen on imaging; many are benign incidental findings, but every image needs the actual radiology report and clinical context.
It is also a reminder that an ugly MRI is not the same thing as an unlivable life. Even with this spine decades later, the author has constant mild pain but still works and rides a bike without relying on strong pain killers; paracetamol/acetaminophen and anti-inflammatory medicines as needed are usually enough. Images matter, but function, adaptation, symptoms and goals matter too.
This is educational imaging, not an online diagnosis for readers. The important question is always whether the MRI finding matches the side, level, nerve pattern, exam findings and timing of symptoms.

Disc surgery options
Disc surgery is usually about decompressing a nerve or spinal cord. It is less predictable when the main problem is vague back pain without a matching compressive lesion.
Timing is one of the hardest decisions. Operate too early and the disc may have settled on its own, making surgery unnecessary. Wait too long with severe nerve compression and weakness, numbness or pain pathways may become harder to reverse. That is why worsening power, progressive numbness, bladder/bowel symptoms and disabling sciatica despite good care change the conversation.
Removes the herniated fragment while leaving most of the disc. Often used for lumbar L4/5 or L5/S1 sciatica after 6 to 12 weeks of failed conservative care, or sooner for major weakness or emergency compression. Cochrane reviews frame the benefit as faster relief for carefully selected sciatica patients, with less certainty about long-term superiority for everyone.
Removes bone and ligament to open the canal, commonly for spinal stenosis. Fusion may or may not be added depending on instability, deformity, slippage or how much bone must be removed.
Anterior cervical discectomy and fusion is common for cervical disc disease with nerve or cord compression. Posterior foraminotomy may suit selected one-sided foraminal stenosis.
Cervical disc replacement can preserve motion in selected patients without major facet arthritis, deformity, instability, infection, osteoporosis or severe multilevel disease. Lumbar artificial discs are more selective and controversial.
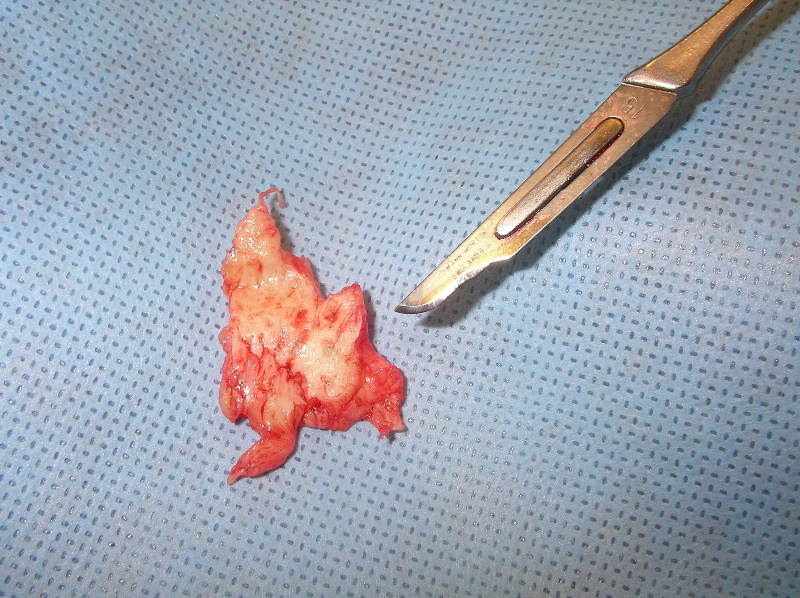
A microdiscectomy removes the fragment that is compressing or irritating the nerve, not necessarily the whole disc. Surgeons usually leave stable disc material behind to preserve as much anatomy as possible.
This kind of image can help patients understand that a herniation is a physical fragment, but it should not be used to compare one patient’s prognosis with another’s.
Modern operating room
Modern disc and fusion surgery can involve smaller corridors, better imaging, nerve monitoring and more sophisticated implants. These tools may reduce tissue disruption or improve precision in selected cases, but they do not make the operation risk-free.
Microdiscectomy uses magnification and small exposures. Tubular retractors and endoscopes can reduce muscle stripping, but the learning curve and case selection matter.
CT navigation, fluoroscopy, O-arm style imaging and robotic guidance can help plan screw trajectories and confirm anatomy, especially in fusion or revision cases.
Somatosensory and motor evoked potentials, EMG and triggered screw testing can warn the team about spinal cord or nerve irritation. Monitoring reduces some risks but cannot prevent every injury.
Modern cages, artificial discs, expandable implants, porous titanium, BMP and graft substitutes give surgeons more options. More options also mean more device-specific questions before consent.
Fusion, cages, grafts and implants
Interbody cages hold disc height and create a space for fusion. They may be titanium, PEEK, carbon-fiber-reinforced materials or porous/3D-printed designs.
Fusion is more likely when there is instability, spondylolisthesis, deformity, severe disc collapse with foraminal stenosis, recurrent herniation with disabling back pain, revision surgery, or decompression that would destabilize the segment. It is less compelling for isolated non-specific back pain.
Artificial discs, gels and regenerative claims
Patients often hear about artificial discs, injectable gels, PRP, bone marrow concentrate, stem cells and exosomes. The right question is not whether the idea sounds advanced, but whether it is approved or regulated for your condition, supported by good outcomes data, and appropriate for your anatomy.
Cervical artificial discs are a mainstream option for selected one- or two-level disease, often C3-C7, when there is no major instability, deformity, severe facet arthritis or osteoporosis. Lumbar artificial discs exist but are more selective, especially when facet pain, spondylolisthesis or multilevel degeneration is present.
Disc gels, nucleus pulposus replacements, hydrogel implants, cartilage-like matrix injections and annular sealants aim to restore disc mechanics, fill a contained defect or reduce re-herniation. They are not a magic rebuild for severe disc collapse, spondylolisthesis, major instability or frank nerve compression. Some are investigational or limited by country, indication and long-term data.
Regenerative injections are heavily marketed for back pain and disc degeneration. Evidence is evolving, but patients should ask whether the product is part of a registered clinical trial, what cells are actually in it, and whether the claim is legal in that country.
Exosome and birth-tissue products are often sold with confident language. In the US, FDA consumer guidance says regenerative medicine products have not been approved for orthopedic conditions including disc disease, back pain or neck pain.
Examples patients may encounter include ReGelTec's HYDRAFIL hydrogel disc augmentation system, DiscGenics' IDCT/rebonuputemcel injectable disc-cell therapy, and VIA Disc NP nucleus pulposus allograft. These examples show the range of approaches: device-like hydrogels, cell therapies, and donated disc-tissue products. They should be discussed in terms of trial status, regulatory approval, eligibility, long-term outcomes and what happens if the injection fails.
Injections and pain procedures
Sometimes. Injections are usually best thought of as diagnostic tools, symptom-control tools, or a way to buy time for natural recovery and rehabilitation. They are less convincing when sold as a permanent fix for a mechanical compression problem.
Often used for sciatica or cervical radicular pain from disc herniation or stenosis. It may reduce inflammation around a nerve root and provide weeks to months of relief, but it does not remove the disc or reliably prevent surgery. Cochrane's sciatica review found only limited support: effects are generally small, short-term and may not be clinically important for every patient.
A targeted injection around one nerve root can help confirm the pain generator when MRI findings and symptoms are complex. Relief after the block can guide surgical level selection, but false positives and temporary relief happen.
If pain is mainly extension/twist-related back pain rather than leg pain, facet joints may be involved. Medial branch blocks can test the diagnosis; radiofrequency ablation may help selected patients for months.
Hip, sacroiliac and muscular pain can mimic disc pain. Targeted injections may clarify the source or reduce pain enough to progress physiotherapy.
Platelet-rich plasma is being studied for tendons, joints and some spine pain generators. For disc disease, evidence and regulation vary; ask whether it is for a disc, facet, SI joint or ligament, and what outcome data support that exact use.
Progressive weakness, cauda equina symptoms, spinal cord compression, severe structural instability or intolerable nerve pain despite appropriate conservative care may move the decision toward surgery instead of repeated injections. Repeating injections without a clear target, objective benefit or rehabilitation plan is often a sign to revisit the diagnosis.
A spinal cord stimulator is an implanted neuromodulation device sometimes considered for persistent neuropathic leg pain after surgery, failed back surgery syndrome or complex regional pain syndrome. It is costly, usually starts with a trial, and is not the same as fixing a disc, fusion problem or unstable spine.
Pain control without pretending pain is simple
Pain control is usually layered: movement, sleep, pacing, physiotherapy, simple analgesia, anti-inflammatory treatment when safe, targeted injections, and only sometimes short-term opioid rescue. The aim is function, not just a lower number on a pain scale.
Getting pain under control early may reduce the chance of fear, guarding, poor sleep, deconditioning and sensitized pain pathways taking over. That does not mean masking red flags or ignoring nerve damage; it means treating severe pain actively while the diagnosis and recovery plan are being clarified.
Paracetamol/acetaminophen may help some people despite weak chronic low-back-pain evidence. NSAIDs such as ibuprofen, naproxen, diclofenac or celecoxib can help inflammatory flares but need stomach, kidney, blood pressure, heart and blood-thinner caution. Topical NSAIDs, heat/ice and short rest can be useful in flares.
Burning, electric or shooting nerve pain may lead clinicians to consider duloxetine, amitriptyline or other neuropathic-pain medicines in selected patients. Gabapentin and pregabalin are controversial for sciatica; NICE advises against gabapentinoids for sciatica because benefit is poor and harms can be significant.
Short courses of muscle relaxants or sedating medicines are sometimes used, but drowsiness, falls, dependence and driving risk matter. Sleep treatment, pacing and anxiety reduction often change pain more than another tablet.
Options include codeine, tramadol, tapentadol, morphine, oxycodone, hydromorphone, fentanyl patches, buprenorphine patches and specialist-supervised fast-acting forms such as sublingual buprenorphine. Constipation, sedation, falls, tolerance, dependence, addiction, hormonal effects and overdose risk are major issues.
CDC guidance says non-opioid treatment is preferred when possible and that acute opioid prescriptions should usually be for the shortest practical duration, often only a few days. Cochrane reviews find no solid placebo-trial support for long-term opioid therapy in chronic low back pain and only small average benefits even where short-term trials exist.
| Adjunct | What it may help | Evidence feel | Practical take |
|---|---|---|---|
| Physiotherapy / physical therapy | Mobility, strength, confidence, recurrence prevention, return to work. | Best-supported non-drug foundation, especially active exercise for chronic low back pain. | Choose an active plan with graded loading, not only passive treatment. |
| Multidisciplinary rehab | Long-term pain, disability, fear, work issues and mood. | Cochrane evidence supports biopsychosocial rehab for chronic disabling low back pain. | Worth considering when pain has become life-limiting or work-limiting. |
| TENS machine | Temporary symptom relief for some people. | Cochrane evidence is uncertain; placebo-controlled benefit is not convincing. | Low-risk trial if inexpensive, but do not build the whole plan around it. |
| Therapeutic / deep ultrasound | Often marketed for soft tissue pain. | Cochrane evidence for chronic non-specific low back pain is weak/uncertain. | Use as an add-on only if it clearly helps you function. |
| Massage and manual therapy | Muscle guarding, short-term comfort, movement confidence. | May help short term; evidence quality varies and effects are usually not curative. | Most useful when paired with exercise and self-management. |
| Acupuncture / dry needling | Some chronic non-specific low back pain and myofascial pain. | Mixed evidence; some reviews find short-term improvement versus no treatment or sham. | Reasonable to trial if safe, affordable and not delaying urgent care. |
| Spinal cord stimulator | Selected chronic neuropathic pain, especially persistent pain after surgery or CRPS. | Cochrane does not support SCS for non-specific low back pain outside trials; evidence is more favorable in selected neuropathic indications but still debated. | Ask about total cost, trial success criteria, battery replacement, infection, lead migration, revision, explantation and what diagnosis it is treating. |
Recovery and outcomes
Walking, wound care, medication taper, avoid bending/lifting/twisting. Some nerve flares are possible.
Light duties may resume after microdiscectomy if pain and job demands allow. Desk work often returns earlier than manual work.
Structured physiotherapy often builds core control, hip strength, gait, and graded return to work. Fusion restrictions usually remain tighter.
Fusion recovery is measured in months. Bone healing, conditioning, and nerve recovery can continue for a year or more.
Tiger Woods had multiple back operations, including an L5/S1 anterior lumbar fusion in April 2017, then won the 2019 Masters. That shows recovery can be extraordinary, but it does not make elite-athlete outcomes the normal benchmark for everyday patients.
The hard consent conversation
A realistic decision is not “surgery good” or “surgery bad”. It is whether the diagnosis, symptoms, neurological findings, imaging, timing, surgeon experience and personal risk profile line up strongly enough to justify the operation being proposed.
Severe sciatica or arm pain eases, walking and sleep return, weakness stabilizes or improves, pain medicines reduce, and work or sport becomes possible again. Many successful patients still need months of conditioning and sensible limits.
The nerve pain improves but back pain remains, numbness persists, the disc re-herniates, stenosis at another level becomes symptomatic, or recovery takes much longer than expected. This is common enough that it belongs in the decision, not as a surprise afterward.
Pain can become worse or chronic. Fusion can fail to unite. Hardware can loosen or irritate tissue. Infection, bleeding, dural tear, nerve injury, foot drop, sexual dysfunction, bladder or bowel dysfunction, paralysis, wheelchair dependence, major medical complications, or death are uncommon but real.
Longer operations, prone positioning, blood loss, frailty, sleep apnea, heart/lung disease, diabetes, anticoagulants and prior anesthesia problems can all change perioperative risk. For a separate patient guide, see AnesthesiaRisks.com.
Provider finder
Choose a care category and enter a city, postcode, country, “near me”, or anywhere you might travel. Links open searches you can refine locally.
For surgical opinions, start with a practising neurosurgeon who regularly performs spinal surgery. Some orthopedic surgeons are dedicated spine surgeons, but many are not. Generic “back clinics”, chiropractic clinics, “spinal adjustment” services and other non-medical providers are not substitutes for a medical diagnosis or surgical opinion when weakness, numbness, stenosis, spondylolisthesis, cord compression or fusion is being considered. People often go there first because access is easy; the risk is losing time when nerve damage is progressing.
Review sites are uneven by country. Use official registers to confirm registration and specialty status, then use reviews, hospital pages and second opinions as extra signals. The same checks matter for locals and for offshore surgery or medical travel; if you cross borders, make the complication and follow-up plan even more explicit.
Back-pain, spinal-fusion and medical-tourism groups can help you learn what questions to ask, what recovery can feel like, and which complications patients worry about. They are also highly anecdotal: dramatic successes and disasters are over-represented, surgeon recommendations may be biased, and paid promotion can be hard to spot. Treat them as lived-experience signals, not proof.
Costs and quote reality
These are rough private/cash or self-pay ranges as of June 2026. Insurance, public systems, complications, implants, hospital tier, number of levels, and exchange rates can change the answer dramatically.
| Country | Discectomy / decompression | Single-level fusion / disc replacement | Best next step |
|---|---|---|---|
| USA | Often USD 10,000-40,000 cash/billed; insured out-of-pocket varies. | Often USD 50,000-200,000+ billed for hospital fusion; implants drive cost. | Ask for CPT codes and use Medicare Procedure Price Lookup plus insurer estimates. |
| UK | NHS usually no direct patient charge; private often GBP 8,000-15,000. | Private lumbar fusion commonly GBP 18,000-25,000+ depending on levels and implants. | Ask if imaging, surgeon, anesthetist, implants and revision coverage are included. |
| Australia | Public Medicare pathway may be low direct cost; private gaps vary widely. | Government-linked cost tools report private fusion ranges around AUD 9,700-18,700+ for many cases. | Use Medical Costs Finder and ask your fund for gap and prosthesis coverage. |
| Singapore | Private sector depends on TOSP complexity, surgeon fee benchmarks and ward class. | Fusion/ADR may add major implant and hospital charges; MOH benchmarks help frame surgeon fees. | Check MOH fee benchmarks and request an itemized estimate before booking. |
| Thailand | Package-style quotes can be around USD 5,000-8,000 for simple single-level cases. | Single-level fusion or cervical disc replacement often starts around USD 7,000-12,000+, more with implants/levels. | Confirm JCI/hospital accreditation, implant brand, follow-up plan, and what happens if complications occur. |
Multilingual quick guide
References and reputable starting points